Good Nutrition is an integral part of an infant’s growth and development
to support the physiological changes that occur during the first year of life.1
A general indicator of an infant’s optimal growth is consuming an
adequate number of calories per day measured as weight for age, length for age and head circumference. In
general, most healthy infants double their birth weight by 6 months of age and triple it by 12 months of
age. An infant’s growth rate can be assessed by periodically plotting the infant’s weight, length, and head
circumference for age and weight for length on World Health Organization (WHO) growth charts throughout the
first year of life.1
Nutrient needs of infants are depending upon the rate of growth, energy
expenditure, basal metabolic needs and nutrients consumed. Macronutrients are needed in larger quantities
(in gram range); they normally include water, carbohydrates, fat and protein.1
Energy
The metabolism of babies and young children differs from that of adults
primarily due to rapid physical growth, changes in organ functions and body composition. Accordingly, a
baby’s daily energy requirements during the first year of life are comparatively high, at around 90 kcal/kg
body weight compared to an adult’s 40 kcal/kg.2,18
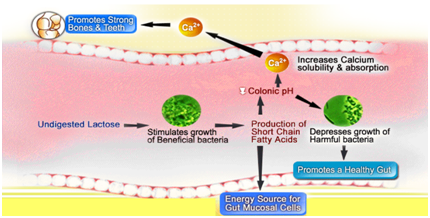
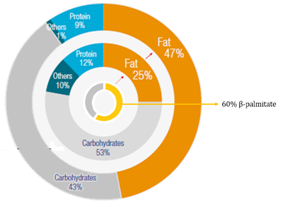
- Carbohydrates supply 30% to 60% of the energy intake during infancy. Approximately 40% of the energy in
human milk and 40% to 50% of the energy in infant formulas is derived from lactose (The most important
carbohydrate in a baby’s diet) or other carbohydrates. Lactose helps with the absorption of calcium,
which is important to bone development.3
- In normal physiological conditions lactose is hydrolyzed to glucose and galactose by lactase also known
as lactase-phlorizin hydrolase, a brush-border membrane-bound enzyme, which is taken up by the
intestinal cells and transported into the bloodstream. Lactose which is not hydrolyzed in the small
intestine is passed into the colon where it is hydrolyzed by the colonic bacterial enzyme
ß-galactosidase resulting in the formation of glucose and galactose. Glucose and galactose are
subsequently converted into lactate as well as into the short chain fatty acids (SCFA) acetate,
propionate and butyrate. These short chain fatty acids lower the intestinal pH leading to increased
mineral absorption of Calcium and Magnesium, hence improves bone mineralization.4
Protein
- Protein requirements during the rapid growth of infancy are higher per kilogram of weight than those for
adults or older children. For infants it ranges from 1.16g/kg/day for the first 6 months to 1.69g/kg/day
for 6 -12 months of age compared to adults 1g/kg/day.18
- Despite protein quantity, protein quality is one of the vital characteristics of the nutritional value
of infant feeding. Human milk that contains predominantly the whey proteins than bovine’s milk is the
gold standard in early infant nutrition.5,6 Human milk contains casein to whey in a ratio of
40:60; while in cow’s milk the ratio is 80:20.
- Casein forms clots or curds in the stomach; while whey remains as a liquid and is easier to digest
& assimilate providing additional energy & sparing endogenous proteins. As cow’s milk is
predominant in casein, its intake results in high curd tension resulting in hard stools and irregular
intake of feed by infants.
- Whey is a rich source of Arginine & lysine which may stimulate growth hormone release, stimulating
an increase in muscle mass & a decline in body fat.6
- Numerous factors affect the quality of proteins; however, the amino acid profile is considered as a
major contributor to overall protein quality. Breast-milk proteins assist in providing adequate
nutrition to breastfed infants while simultaneously aiding in the defense against infection and
facilitating optimal development of important physiologic functions in newborns. Indian Academy of
Pediatrics recommends that exclusive breastfeeding should be practiced till the end of six
months.16
Fats
- Up to 98 % of human milk lipids are in the form of triacylglycerols, in which saturated and
non-saturated fatty acids are bound to the skeleton of glycerol.
- Palmitic acid, the major saturated fatty acid in human milk, usually represents about 20–25 % of human
milk fatty acids. 60% of which is esterified to the sn-2 position in the triacylglycerols (the so-called
ß-position).7-9
- If infants are fed with fats containing mainly palmitic acid located in the sn-2 position, leads to
higher absorption and efficiency of palmitic acid in comparison with supplemental milk formulas with
triacylglycerols derived from vegetable oils that are predominantly in the sn-1 and sn-3
position.10
- If palmitic acid is bound in the sn-2 position to glycerol, it does not create compounds with calcium,
but is absorbed thereby positively influencing mineralization of the growing skeleton.
- Cow’s milk, as well as plant fats, have lower content of ß- palmitate compared to human milk (cow’s milk
only about 40 %, plant oils even only 5–20 %).11
- According to the available data, ß-palmitate positively influences fatty acid metabolism, increases
calcium absorption, improves bone matrix quality and the stool consistency, and has a positive effect on
the development of the intestinal microbiome.19
Micronutrients
Calcium, Phosphorus & Vitamin D
- Early childhood is critical for the optimal development of bone matrix mineralization and diet
significantly influences this complex process.1
- Vitamin D deficiency is growing in India among all age groups, and Indian children in general have been
reported to consume insufficient calcium. This, in addition to Indian’s changing lifestyle and lack of
fortification, led IAP to create a practice guideline for pediatricians in order to prevent and treat
vitamin D and calcium deficiency.12
- Studies were conducted in the age group of new borns up to 6 months and showed prevalence from
62-95.7%. These studies have revealed predisposition of lower 25(OH)D concentrations to neonatal
hypocalcemia and infantile rickets with biochemical evidence of hyperparathyroidism among infants
manifesting with hypo-calcemic seizures with Vitamin D deficiency. The Significant association between a
deficient Vitamin D status (45.5%) and low birth weight has also been observed.12,13
- Studies were mainly conducted in the age group of 9 months -5 years with the prevalence of
46-80%.14
- The calcium content of cow’s milk (120mg per 100ml) is nearly four times that of human milk (34mg per
100ml). Although human milk contains less calcium, it is more easily absorbed than that found in cow’s
milk.
- EFSA (2005) states 1.5:1 is optimum Ca:P ratio for infants. A meta -analysis showed average Ca:P ratio
in human milk is 1.7:1.22
- Vitamin and mineral supplements should be prescribed only after careful evaluation of the infant’s
intake. Commercially prepared infant formulas are fortified with all necessary vitamins; therefore
formula-fed infants rarely need supplements.1
Iron
- 82% of Indian children under age of 6-23 months consume less than the recommended amount of Iron and
thus the high prevalence of Iron deficiency Anaemia. Only 17.9% of Indian children under age of 6-23
months consume Iron rich food daily.15
- Iron forms traditionally used in food manufacturing have low bioavailability. Heme (organic) iron,
found in meat, and non-heme (inorganic) iron each have a different transporter in the gut. Non-heme iron
consists of both ferrous (Fe2+) and ferric (Fe3+) forms, and is the main source of iron compounds used
in food fortification.
- Healthy breastfed infants absorb iron well from human milk and usually maintain normal iron stores
during the first 4 to 6 months. However, the bioavailability of iron in cow’s milk is much less than
human milk. Thus, cow’s milk consumption in infancy associated with an increased risk of developing
Fe-deficiency anaemia.16, 20
- Formula-fed infants up to 6 months of age should receive iron fortified infant formula, with an iron
content of 4 to 8 mg/L. Follow-on formulas should also be iron fortified; however, there is not enough
evidence to determine the optimal iron concentration in follow-on formula. 21
- In case the above is not possible, Iron supplementation should be advocated.
Zinc
- Zinc is one of the trace elements that can become limiting for exclusively breastfed infants. In
contrast to Iron, the requirements are quite high initially (2-3 mg/L) that declines rapidly in the
first few months of life and more rapidly around 4 months postpartum.
- Many intervention trials have been conducted in many countries to assess the effect of zinc
supplementation on children’s growth, with positive outcomes.
- The EC Directive guidelines recommend a zinc concentration of 300-750 mcg/100 ml formula for term
infants.20
References:
- Mahan et al., Krause’s Food and Nutrition Therapy. 12th Edition. Chapter 6: Nutrition during
Infancy. Pg. 199-221.
- Druet C, Stettler N, Sharp S, et al: Prediction of childhood obesity by infancy weight gain: an
individual level meta-analysis, Paediatr Perinat Epidomiol 26:19–26, 2012.
- Mahan et al., Krause’s Food and Nutrition Therapy. 14th Edition. Chapter 16. Nutrition in Infancy.
- Vonk R. et al., Chapter 7: Probiotics and Lactose Intolerance. http://dx.doi.org/10.5772/51424
- Zhang Z, Adelman AS, Rai D, Boettchar J, Lonnerdal B. Amino acid profiles in term and preterm human
milk through lactation: a systematic review. Nutrients. 2013;5 (November (12)):4800–4821.
- Luque V, Closa-Monasterolo R, Escribano J, Ferré N. Early programming by protein intake: the effect
of protein on adiposity development and the growth and functionality of vital organs. Nutr Metab
Insights. 2016;8(March (suppl 1)):49–56.
- Innis SM, Dyer R, Nelson CM. Evidence that palmitic acid is absorbed as sn-2 monoacylglycerol from
human milk by breast-fed infants. Lipids. 1994;29:541–5.
- Lopez-Lopez A, Castellote-Bargallo AI, Campoy-Folgoso C, Rivero-Urgel M, Tormo-Carnice R,
Infante-Pina D, Lopez-Sabater MC. The influence of dietary palmitic acid triglyceride position on
the fatty acid, calcium and magnesium contents of at term new born faeces. Early Hum Dev.
2001;65(Suppl):83–94.
- Straarup EM, Lauritzen L, Faerk J, Hoy CE, Michaelsen KF. The stereospecific triacylglycerol
structure and fatty acid profiles of human milk and infant formulas. J Pediatr Gastroenterol Nutr.
2006;42:293–9.
- Carnielli VP, Luijendik IHT, van Goudoever JB, Sulkers EJ, Boerla AA, Degenhart HJ, Sauer PJ.
Structural position and amount of palmitic acid in formulas: effects on fat, fatty acid, and mineral
balance. J Pediatr Gastroenterol Nutr. 1996;23:554–60.
- Tomarelli RM, Meyer BJ, Weaber JR, Bernhart FW. Effect of positional distribution on the absorption
of the fatty acids of human milk and infant formulas. J Nutr. 1968;95:583–90.
- Khadilkar, et al., Prevention and Treatment of Vitamin D and Calcium Deficiency in Children and
Adolescents: Indian Academy of Pediatrics (IAP) Guidelines. Indian Pediatrics. VOLUME 54__JULY 15,
2017
- Surve S, et al., Review Article: Vitamin D deficiency in Children: An update on its Prevalence,
Therapeutics and Knowledge gaps. Indian Journal of Nutrition. Volume 4, Issue 3 – 2017.
- National Family and Health Survey 2015-16
- Griebler U et al 2015., Health effects of cow’s milk consumption in infants up to 3 years of age: a
systematic review and meta-analysis. Public Health Nutr. 2016 Feb;19(2):293-307.
- Tiwari S, et al., Infant and Young Child Feeding Guidelines, 2016. VOLUME 53__AUGUST 15, 2016
- Thomas E, et al., Biochemistry, Iron Absorption. Available at:
https://www.ncbi.nlm.nih.gov/books/NBK448204/#article-23766.s1
- RDA 2010, NIN, ICMR 2011
- Havlicekova Z., et al, Review: Beta-palmitate – a natural component of human milk in supplemental
milk formulas. Nutrition Journal (2016)
- Fewtrell M et al, Chapter 16: Infant Feeding. Page no. 281-324
- Magnus D, et al., Iron requirements of infants and toddlers. Journal of Pediatric Gastroenterology
and Nutrition, 58(1):119-129
- Dorea J, et al., Calcium and phosphorus in human milk. May 1999 Nutrition Research 19(5):709-739